Ligaments are structures in the body that connect one bone to another bone. They allow our joints, such as our knee joint, to move while providing it some stability. We have two cruciate ligaments in each knee, the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL). They are situated in the middle of our knees connecting our femur and tibia bones together. The ACL provides stability to our knee when we twist and pivot during daily activities and strenuous sports.
The ACL itself is an extremely strong structure but can still tear or rupture if excessive force is applied to it! This happens in sports that involve sudden changes of direction at speeds while the foot is firmly planted to the ground; football, basketball, and skiing, to name a few. Some athletes sustain an ACL rupture due to a direct blow to the knee or a collision such as a football tackle. We can still walk and run even without an intact ACL, but our knees may not be able to tolerate pivoting movements.
Let’s look at the ACL in a little more detail to understand its structure and function in our knees!
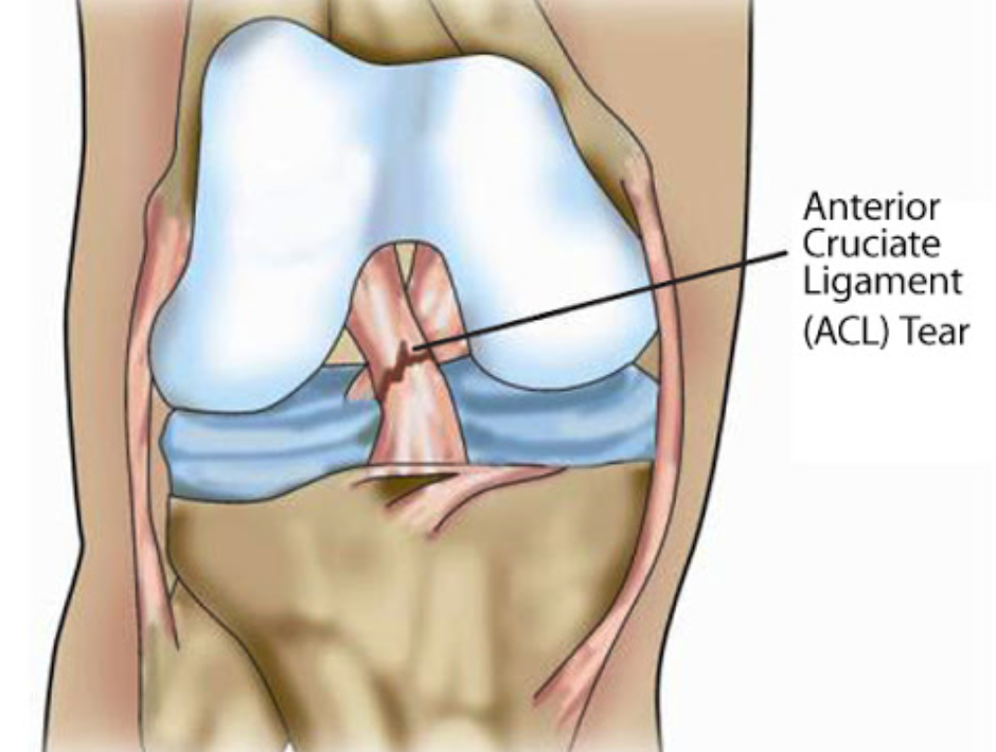
Explanation of the ACL (anterior cruciate ligament) and its role in knee stability
As mentioned above, the ACL is a ligament in the knee which connects the femur bone to the tibia bone. They act firmly like a rope holding two boats together. The ACL ensures that the femur and tibia bone do not move too far apart or twist too much during strenuous physical activities. There are other ligaments in the knee, such as the medial and lateral collateral ligaments (MCL, LCL), which also provide stability to the knee but in different directions. Studies have shown that it requires between 2900 Newtons of force to over 7000 Newtons of force to actually rupture an ACL (Boden et al, J Am Acad Orthop Surg 2013).
Prevalence of ACL injuries in skiing
Ligament injuries are very common in skiers. It was reported that ACL and MCL injuries make up about 25% to 30% of all skiing injuries. This includes both amateur and professional skiers. So why is it so common? Unlike snowboarders, skiers' feet are independently attached to two separate skis through their rigid ski boots. While skiing at high speeds and torque, skiers may lose control of their feet, and both feet may move uncontrollably in very separate directions. One knee may twist hard while the skier’s body tumbles down the side of the mountain. If the twisting force is more than what the ACL can tolerate, the ACL will rupture, and the skier will experience immediate pain in the knee.

The other mechanism by which skiers may rupture their ACL is through the ‘anterior drawer’ method. As they land off balance and their buttock hits the slope, their lower leg in the boot continues to move forward. This pulls the ACL forward to the point of rupture. Sometimes the fall while skiing is so bad that the ACL injury may be the result of a combination of twisting movements!

Overview of ACL reconstruction surgery as a common remedy for skiers. Preventing ACL Injuries in Skiing
Risk factors specific to skiers (equipment, technique, conditions)
There are some ways to prevent serious knee injuries while you ski. With any sport that requires equipment and training, it is important to inform the professional at the ski rental shop of the level of your skiing abilities (beginner, intermediate, professional). For beginners who are more likely to fall while skiing and who have not formed protective mechanisms when they fall, the fitters may adjust how tight your skis attach to your ski boots and make them slightly looser. This allows the skis to disengage from the boots when you fall so that the high torque or twisting forces are not translated to your knee to cause those ligament injuries. The drawback of this is that each time you fall and your skis disengage, you will have to walk down the slopes in your chunky ski boots to pick up your skis.

Professional skiers, on the other hand, will want a very tight attachment between their ski boots and their skis to prevent any disengagement as they travel downhill at high speeds and carve the mountain at high torques! They will NOT want their skis to disengage!

Beginners or intermediate skiers should also undergo some training with a certified coach to learn the basics of skiing downhill safely to prevent serious injuries. This is especially true for skiers who ski only once a season.
Immediate steps following an ACL injury while skiing
When a skier sustains a serious twisting knee injury, it is often difficult to assess what the injury actually is. This is because of the multiple layers of clothes the skier is wearing. It may only be after the skier returns to their cabin that they may find their knee to be swollen and painful. They may also not be able to ski any further as the knee is too unstable and unable to tolerate any further weight or twisting. When this happens, it is best to stop skiing for the rest of the trip and apply some compression and ice to the injured knee. The doctor or medical personnel in the ski village may be able to organize an x-ray for you just to ensure that there are no fractures (broken bones) or knee dislocations. If you require an MRI scan to confirm the extent of ligament injuries, you may have to organize it in your home country or at a hospital or medical facility in a bigger city. You should seek the help of an orthopaedic surgeon or sports doctor if you suspect you may have torn your ACL or any other ligament in your knee.
The Road to Recovery: ACL Reconstruction Surgery
Goals of surgery (restoring stability, preventing further damage)
As an orthopaedic surgeon, I see patients with ACL ruptures all the time. Some may see me within hours of the injury, while others see me several weeks after. It is important to resuscitate the injured knee for several weeks with ice, compression and physical therapy so that it does not become painful and stiff. If the MRI scan or clinical examination confirms the ACL rupture, I usually have a long conversation with the patient to decide which is the best conservative or surgical option for him/her. Patients with torn ACLs may still participate in linear activities where they move in one direction without their functioning ACL. An unstable knee may also lead to further injuries to the meniscus and cartilage.
Completely torn ACLs do not regenerate as their blood supply (from branches of the middle geniculate artery) is lost. Reconstructive surgery is aimed at recreating a new ACL from a graft so that the knee regains its stability and patients may return to their active lifestyle without having to worry about their knee giving way.
Description of ACL reconstruction surgery (graft choices, procedure)
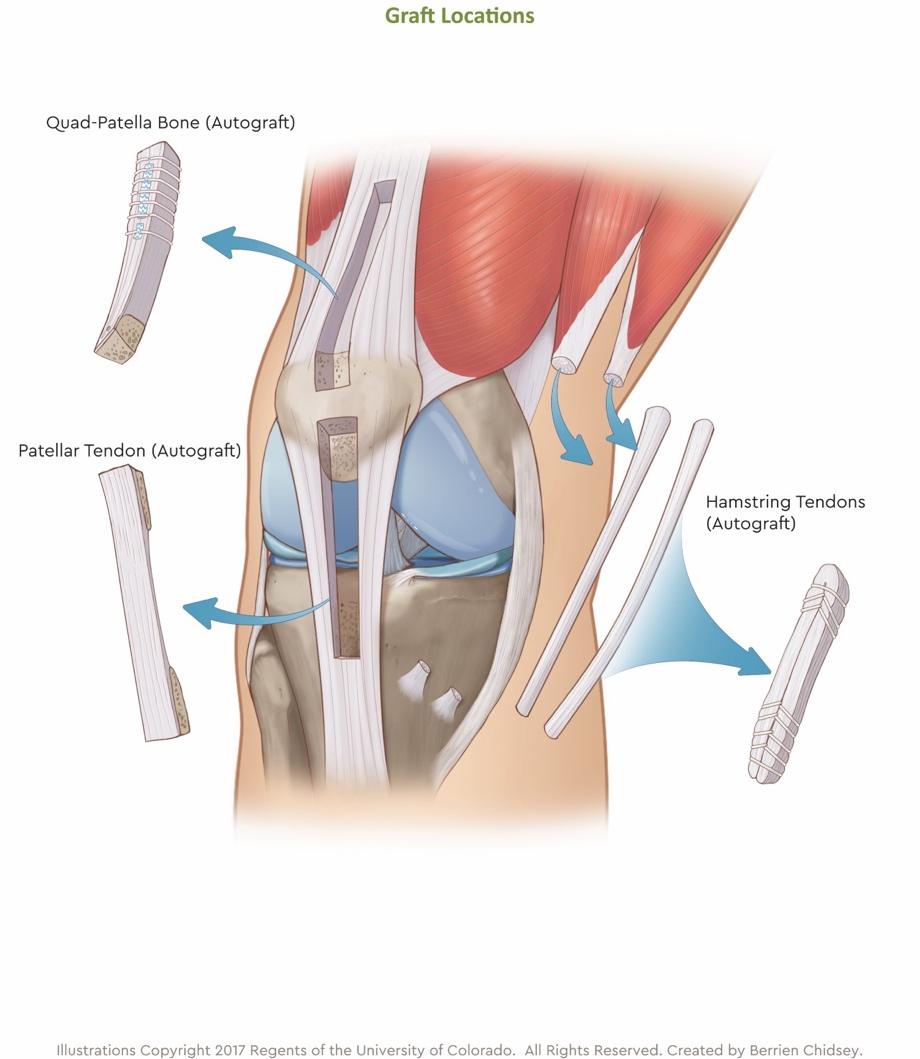
There are several ways that a new graft for the surgery may be obtained. It may be obtained from the patient themselves (autograft) or from a cadaver (allograft). Many factors must be considered before an orthopaedic surgeon decides which option is best suited for the patient. Factors to consider include patient's age, whether this is the first ACL surgery or not and cost. Patients below the age of 25 should avoid using cadaveric allografts for their surgery as these grafts are associated with higher failure rates (higher risk of re-rupture). This is most likely due to the irradiation that these cadaveric allografts undergo to ensure they do not harbour any infection. Despite this risk of re-rupture, patients undergoing revision ACL surgery tend to receive cadaveric allografts as they may already have used their own grafts in their first surgery. They may also not want to undermine their knee any further by harvesting yet another autograft.
For patients receiving their own autografts, their surgeon may opt to use one of several options (hamstring, patella tendon, quadriceps tendon). This may depend on the age of the patient, the urgency to return to sports and the surgeon’s usual practice. The size of the graft harvested must also be big enough for the patient so that it does not re-rupture. Grafts smaller than 8mm in diameter have higher rates of rupture. Dr Mizan usually harvests the patients’ hamstring when performing ACL reconstruction surgery. If one hamstring (semi-tendinosus) is more than 24cm across and may be folded to produce a graft diameter of more than 8mm across, a second hamstring (gracilis) is not required. In smaller patients, Dr Mizan may harvest both the semi-tendinosus and gracilis to produce a robust graft of more than 8mm in diameter. Patella and quadriceps tendon grafts are associated with some anterior knee pain around the patella; hence this is not the preferred option for Dr Mizan. About 80% of the hamstring regenerates by 12 months, and the initial loss of strength is made up by rehabilitation and physiotherapy after surgery.
Post-operative care (immediate care, rehabilitation timeline). Rehabilitation and Physical Therapy
The Importance of Physical Therapy in Recovery
Rehabilitation and physiotherapy after surgery are just as important as the surgery itself. Patients may even start therapy before their surgery if their surgeon feels that their muscle strength or range of motion is lacking. Accelerated rehabilitation is the buzz term for patients to get them moving early and prevent the knee joint from stiffening and muscle from weakening.
Physical therapists ensure that patients go through the various stages of their rehab at the appropriate speed using modern technologies and equipment so that their graft may heal well in their knee, the function and strength of the knee improves and they return to sports in a safe way. Let’s now go through the various phases of the rehabilitation after ACL surgery.
Phases of ACL rehabilitation (early motion, strength training, functional exercises)
The aim of the first two weeks after surgery is to reduce swelling and minimise pain around the knee as well as increase the range of motion of the knee itself. Physios do this with icing, compression, massage and mobilisation/strengthening exercises. Excessive and stressful movement of the knee is not encouraged as this has a negative effect on the healing of the new graft to the bone surrounding it (ACL graft-bone tunnel incorporation).

Between three and five weeks after surgery, physios continue to improve the range of motion of the knee as well as improve the gait or walking pattern of patients. They do this through strengthening exercises as well as balance/proprioceptive training, where patients balance on one leg as they negotiate standing/squatting movements.
Further strengthening and balance exercises are beyond 2 months post operation to allow patients to return to linear sports such as jogging, cycling and swimming. Patients must exhibit a full range of motion of their knee and must not have any knee instability as they perform various exercises. When athletes return to sport between two and 5 months after surgery, physios ensure they have passed a running, agility and plyometric program. They must also have passed a functional assessment where the strength and function of their operated leg are compared to their unoperated leg.
Pivoting sports should be avoided for 10 to 12 months after surgery to allow further healing and prevent re-rupture of the graft. This may occur as the graft undergoes remodeling after surgery and may be weak.
Customised rehab programs for skiers
About 30% of patients re-rupture their ACL within two years of surgery. It is, therefore, important that patients undergo comprehensive physical therapy before they return to the slopes. Patients are encouraged to speak to their orthopaedic doctor to discuss their condition, as the doctor would be familiar with the injury/injuries and the stability of the knee after surgery.
ACL rehabilitation for skiers wishing to return to the slopes should include the following:
- One-legged balance exercises (strength, stability of the knee)
- Hip and thigh exercises: the muscles below and above the knee should be strong enough to protect the knee
- Core exercises: your core helps to maintain balance while you carve the slopes without putting too much strain on the knee.

Return to the Slopes: Criteria and Consideration
Functional tests and criteria for return to skiing
As mentioned above, physical therapists will ensure that patients have good strength and balance in their injured leg and are able to perform repetitive stress tests at speed. This includes running side to side, forward, then backwards running, running in constantly changing directions and performing one-leg squats. Patients are encouraged to maintain their general fitness and flexibility as well as improve their skiing technique to help prevent further injuries.
Equipment modifications and protective gear post-surgery
It is also important to check on your equipment, such as the size and rigidity of your ski boots, the length and width of your skis and how tight the boot is attached to the skis. The professional at the ski rental shop may loosen the attachment so that the skis disengage easily when you fall. This prevents a serious twisting force to your knee and helps prevent re-rupture of the ACL. You are also advised to wear a simple compression brace around your knee for added protection.
Psychological readiness and overcoming fear of re-injury
When returning to skiing after an injury, it is best to start with gentler slopes and limit your ski time to something that is manageable and non-exhausting. If your muscles are not prepared for such strenuous activities, muscle fatigue may set in and cause a fall. Do not ski alone. Have a friend, family member or an instructor ski with you so that they may look out for you in case of a fall. If you do end up falling, remember to keep your legs flexed and fall forward. This helps to reduce the force on the ACL graft and prevents re-rupture.
Skiing is an enjoyable sport. It is not necessary to be there at the first and last ski lifts of the day. Perhaps spend a couple of hours skiing and use the rest of the day taking in the beautiful scenery around you or perhaps have a hot chocolate at a nearby cabin. This helps to reintroduce the joy of skiing and overcome the fear caused by the fall last season. Take beautiful photos and videos and share them with your loved ones on social media!
Conclusion
Summary of the importance of proper treatment and rehabilitation for ACL injuries in skiers
ACL injuries may happen while you ski, and it does not spell the end of your skiing ambitions. It is important to seek medical attention from an experienced orthopaedic doctor or surgeon so that ACL reconstruction surgery may be performed timely. Physical therapy is extremely important for your functional recovery so that you may return to skiing by the following season.
Accelerated rehab using modern equipment and protocols helps you regain your range of motion as well as strength and balance.
Encouragement for a cautious and informed return to the sport
While we all want to return to skiing sooner rather than later, it is important that we have passed the necessary functional and physical tests to assess our leg strength, balance and agility. Going slow using the appropriate equipment is also important to reintroduce us to the sport that we love. Confidence will grow with time and so will the enjoyment as you carve the snow on the slopes. Ski in a group so that your loved ones or ski instructor may look out for you while your skiing.
Finally, enjoy skiing! There’s nothing quite like it!