Orthopaedic conditions encompass a wide range of ailments that affect our musculoskeletal system, often leading to discomfort and reduced mobility. In this article, we will delve into some of the most prevalent orthopaedic conditions, including osteoarthritis, fractures, strains and sprains, and tendonitis. Understanding and recognising these common issues is not just a matter of comfort; it's a key factor in effective treatment and prevention. Timely identification and comprehension of these conditions can mean the difference between swift recovery and long-term complications. From the slow, grinding pain of osteoarthritis to the sudden trauma of fractures or the discomfort and limitations caused by strains and sprains, these conditions can be both physically and emotionally challenging. By gaining insight into the nature of these issues, we empower ourselves to seek appropriate care, make informed decisions, and take preventative measures to ensure a healthier and more active life.
Osteoarthritis
Definition and Overview
Osteoarthritis of the knee is a degenerative condition where the protective cartilage covering our knee joints is worn out and no longer provides the smooth, protective surface for our joints to move. Patients start to develop pain, stiffness and loss of function, which affect their daily activities. They may start to limp and change their activities to cope with the pain. Some even start to develop deformities of their legs, such as bow-leggedness and knock knees. Millions of people around the world are affected by knee arthritis, impacting their basic quality of life and happiness.
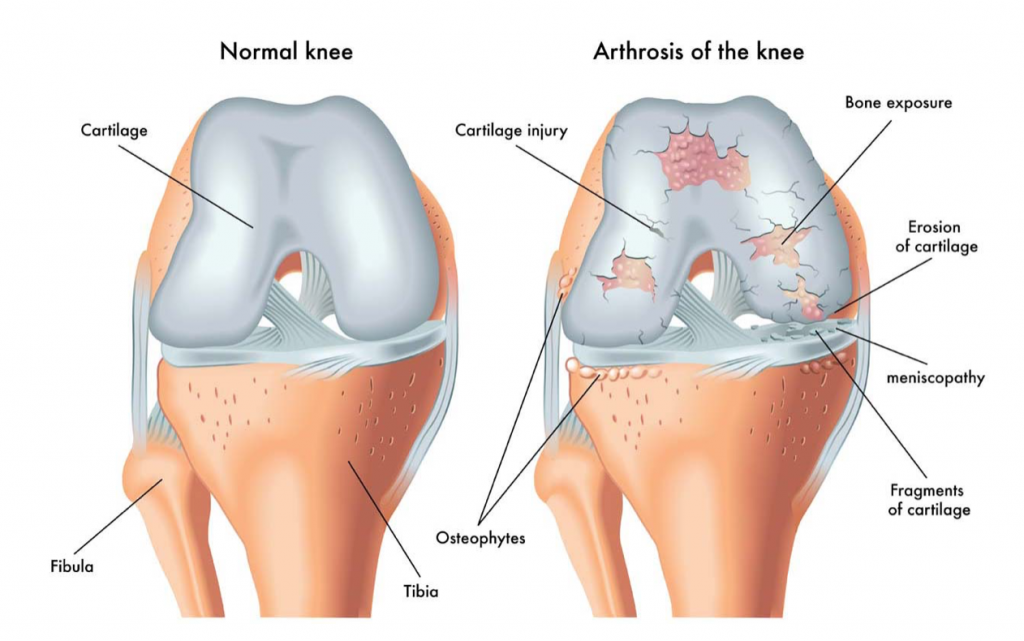
Features of knee arthritis
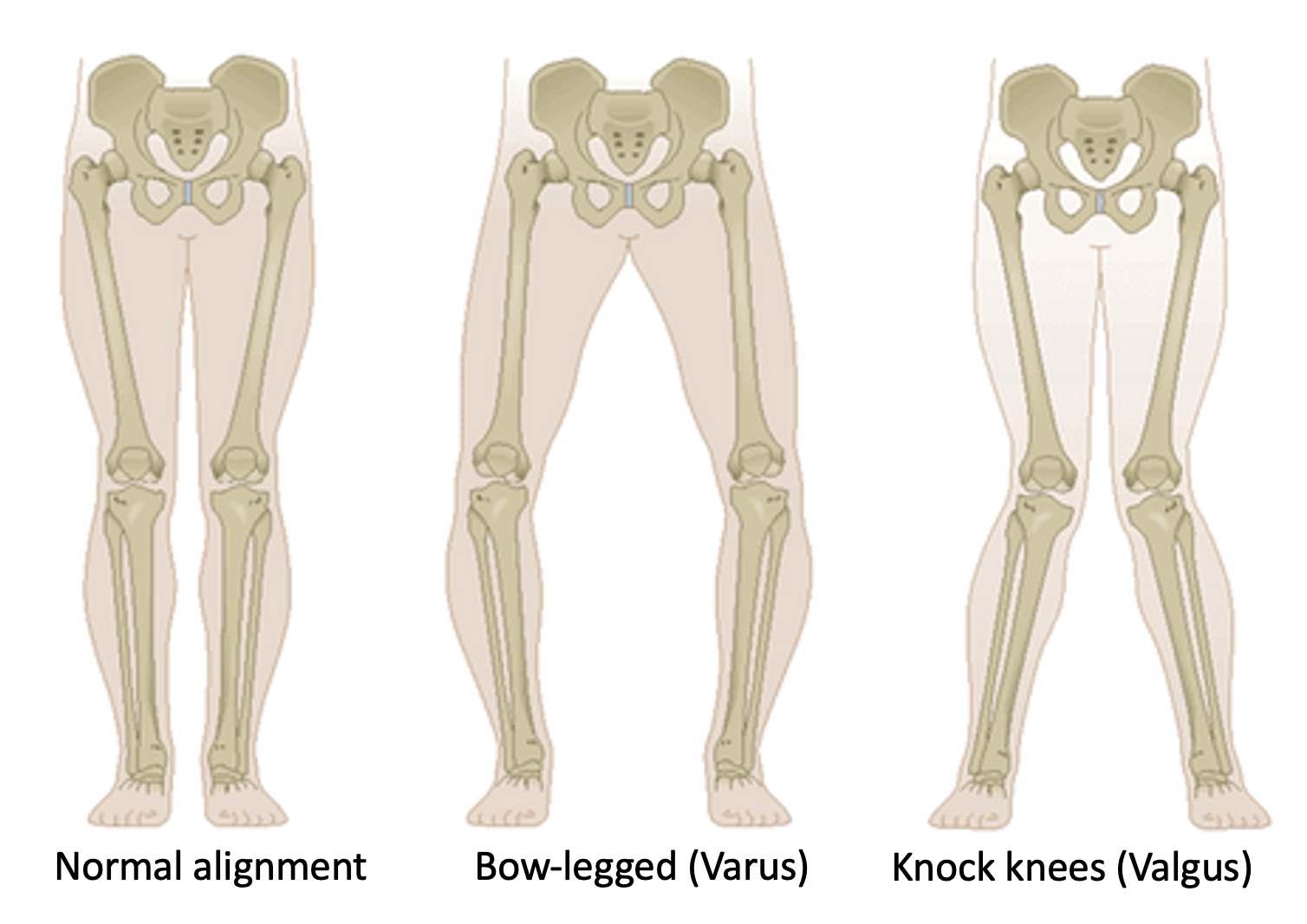
Different lower limb alignments
Causes and Risk Factors
Osteoarthritis is a degenerative process related to age, physical activities, genetics and patient body mass. Inflammatory arthritis, such as rheumatoid arthritis, ankylosing spondylitis, gout, and psoriatic arthropathy, describes an autoimmune condition where the body fights itself and causes degeneration of multiple joints around the body at a younger age.
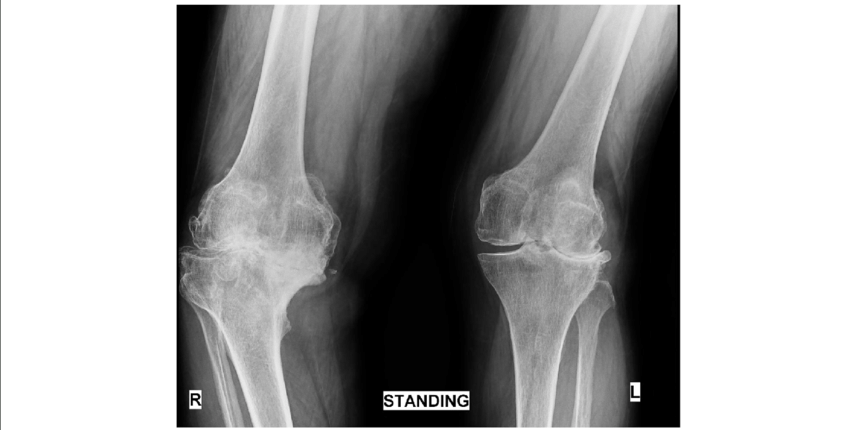
X-ray of a patient with rheumatoid arthritis: the right knee is in varus while the left knee is in valgus (wind-swept knees). There is severe loss of joint space in both knees, with the right knee being significantly worse than the left.
Symptoms and Progression
In the early stages of arthritis, patients may experience intermittent pain, which may come and go with certain activities. Knee pain may be accompanied by swelling, stiffness and gradual deterioration of function. Patients may find themselves limping or walking with an unusual gait to overcome their pain. In the later stages of arthritis, patients may find that they have become bow-legged or knocked-knees. If symptoms become too severe, many middle-aged patients choose to quit their jobs or retire early as the pain becomes overwhelming.

Knee pain from arthritis may affect middle-aged and elderly patients.
Diagnosis (including imaging and physical examination)
The diagnosis of osteoarthritis may be made by the following:
- Most doctors, physicians and surgeons would take a thorough medical history to determine details about the knee pain: duration, severity, what factors make it better or worse, associated symptoms, effect of arthritis on personal and professional life).
- A simple x-ray is performed with the patients standing up to determine the alignment of the knees from the front, the side, and the top (skyline view of the patella). These different views of BOTH knees, while the patient is standing, will give information about the alignment of the knees when patients are standing and which of the three knee compartments is worn out.
- If X-ray images are not conclusive enough, an MRI scan of the knee is organised to assess cartilage wear, meniscus tear and integrity of the different ligaments in the knee.
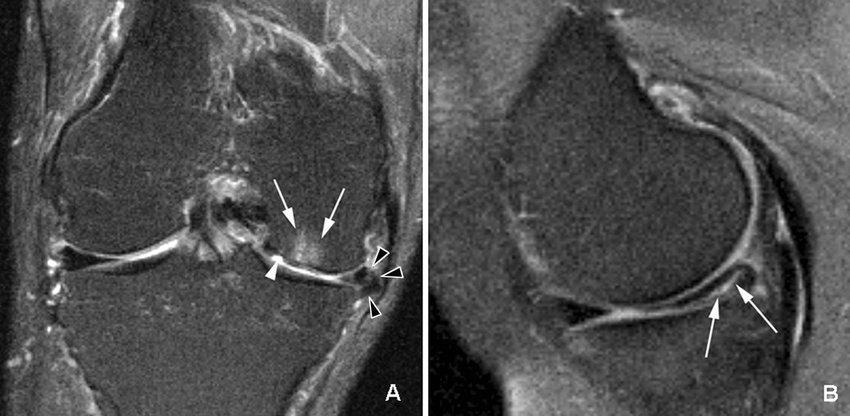
MRI scan of a knee showing bone marrow oedema and cartilage loss (figure A) and a meniscus tear (Figure B)
Treatment Options
- Non-surgical approaches (medications, physical therapy, lifestyle modifications)
Most patients get better with simple treatment such as rest, modifying their physical activities and physiotherapy.
Most will require simple analgesia such as anti-inflammatory medications (Arcoxia, Diclofenac) and oral paracetamol.
We usually send patients for physiotherapy and rehab to strengthen their lower limbs, stretch out certain muscle groups which are tight and improve their gait and balance.

Quads strengthening exercises help with knee pain
- Surgical interventions (joint replacement, arthroscopy)
In the early stages of arthritis for younger patients, the idea of surgery is to preserve their knee and improve their physical function. Some minimally invasive surgical techniques are performed to restore their torn cartilage as well as to repair any torn meniscus. The menisci are two very important shock absorbers in the knee, and their integrity must be restored so they may continue to protect the cartilage.
Some patients have malalignment of their legs, which causes cartilage and meniscus in different parts of their knee to wear out faster. This is similar to the tyres of a car, which are malaligned. The tyres may wear out much quicker than the manufacturer promised! If patients have lower limb malalignment, a different orthopaedic operation may be performed to realign the bone. This is called a corrective osteotomy.

A distal femur osteotomy is performed to straighten a valgus knee

A high tibial osteotomy (HTO) is performed to straighten a varus knee
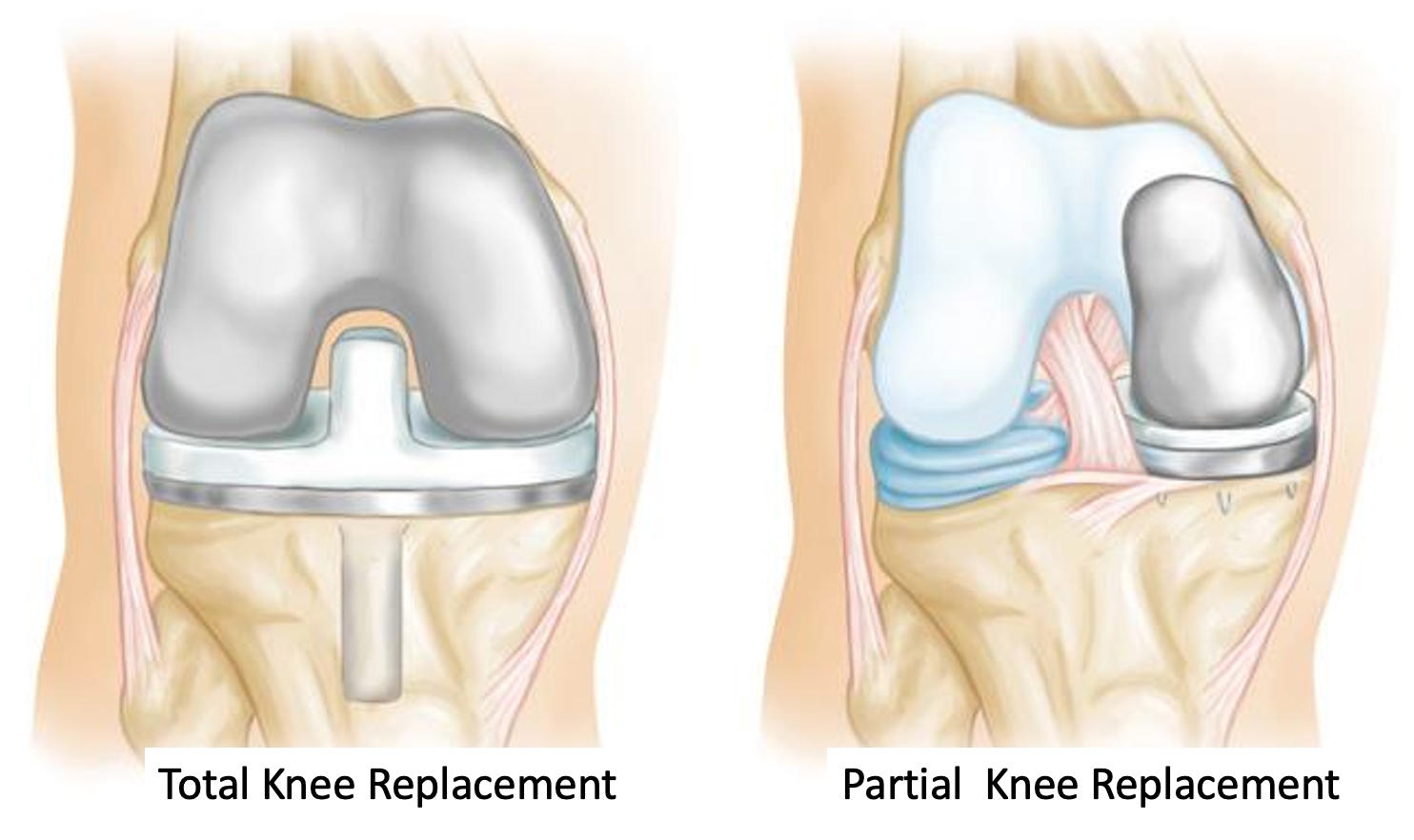
If patients are middle-aged and the condition of their knee is too severe to repair, they may then benefit from replacement surgery. There are partial as well as total knee replacements performed for such patients. The decision depends on multiple patient factors such as age, body weight and integrity of their ACL. Your orthopaedic surgeon will go into greater detail about the pros and cons of both types of knee replacement surgery and which one would suit you best.
Fractures
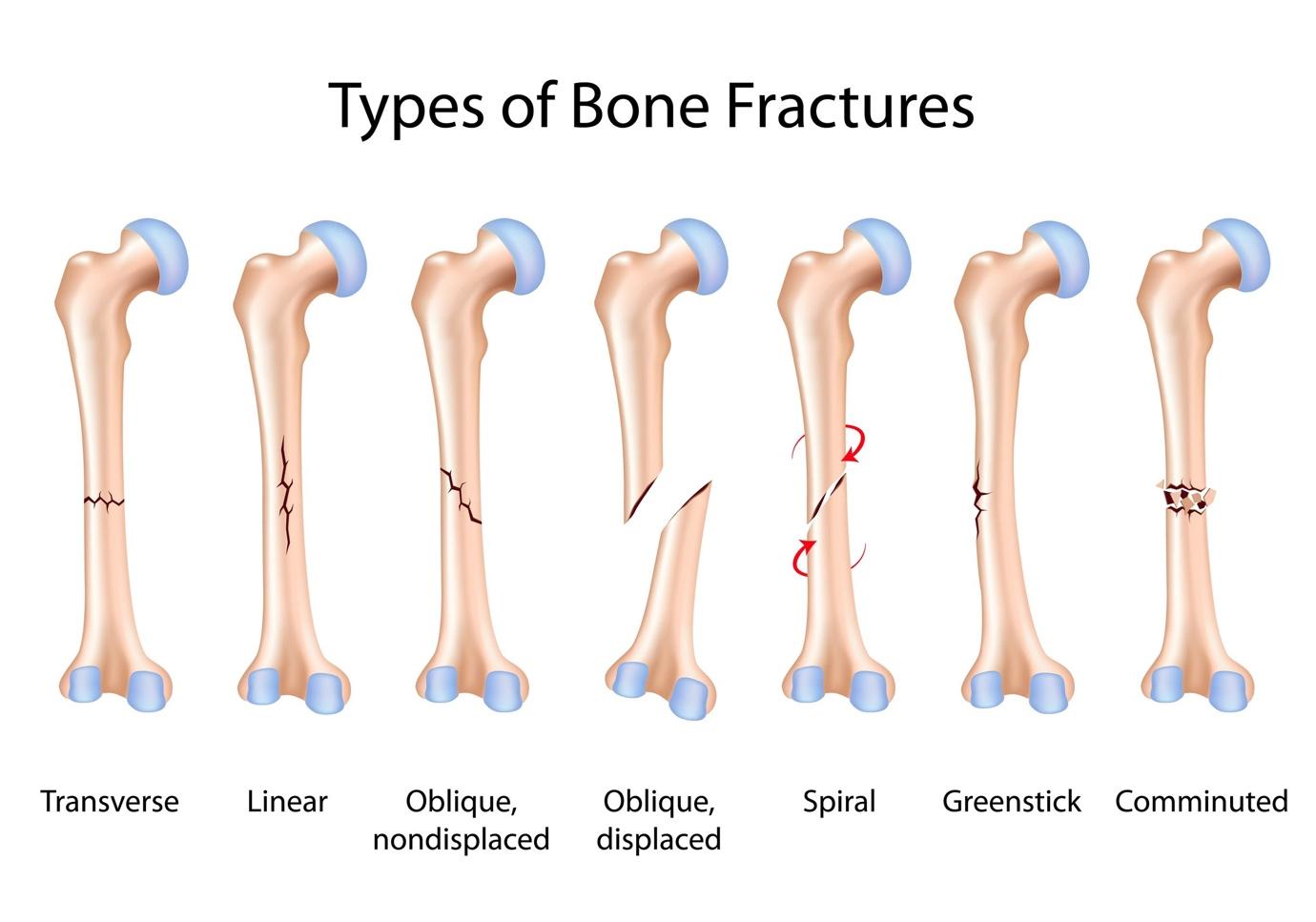
Types of Bone Fractures (open, closed, stress fractures, etc.)
A fracture is a break in a bone. Fractures may be described in many ways to illustrate the extent of the injury, how it came about and whether they are associated with other injuries, such as nerve and skin injuries.
Hairline or undisplaced fractures mean that the bone is broken but has not shifted. Simple fracture describes a single break in the bone, while complex fracture means that the bone is broken into many pieces.
Closed fractures mean that the overlying skin and soft tissue envelop are intact. In contrast, open fractures mean that the broken bones are exposed to the elements because the overlying skin has been breached, and bacteria from the environment may infect the fracture site.
Most fractures happen due to a fall or trauma (road traffic accidents, falls from height). There are also other fractures that occur due to overuse or repetitive motions. Such fractures include stress fractures of the foot in soldiers who march long distances or long-distance runners. Pathological fractures occur due to problems with the bone itself. These include patients with osteoporosis or where cancer has spread to the bone.
When patients present to a fracture to any bone, the medical practitioner will take a thorough history from the patient or loved ones to find out the mechanism of injury, when the injury occurred and if there are associated injuries elsewhere. The past medical history of the patient must be sought to exclude any history of metabolic bone disease, malignancy or risk factors such as smoking and alcohol consumption. A clinical examination is performed to assess the injured area for integrity of the soft tissue, associated nerve or vascular injuries and the function of the injured limb. A basic x-ray examination is performed to determine the location and severity of the fracture before appropriate treatment is given to the patient.

X-ray shows a simple spiral fracture of the mid-tibia bone
Causes and Risk Factors of Bone Fractures
Most fractures occur due to a mechanical injury, such as a fall. Patients fall for many reasons. External environmental reasons include poor lighting, cluttered walking surfaces, uneven ground or a push from someone while walking. Patient factors include medical conditions such as poor eyesight, poor balance, weak muscles or joint pain, which make walking unsafe. Patients with metabolic bone disease such as osteoporosis may experience fractures of their spine without any major injury as their bones are extremely brittle. Elderly patients with certain medical conditions may faint or fall from lower blood pressure, dizziness or a heart arrhythmia. They may then suffer a fracture as a result of the fall.

Falls are especially common in the elderly with medical conditions
When medical practitioners assess patients with fractures, a thorough conversation should include patients’ past medical history, medication history, and social history, such as occupations and sports, as well as a detailed understanding of how the patient may have sustained the fracture. For middle-aged patients, malignancy must be excluded, especially if there was no fall to have caused the fracture in the first place.
Symptoms and Diagnosis of Bone Fractures
Most patients with a fracture will experience pain. There may be associated swelling and loss of function in the initial phases of the injury. A simple X-ray analysis of the affected limb will give the clinician an idea of the severity of the fracture and what the treatment of it should be.
Sometimes, we see other features on the X-ray that make us worry about pathological fractures, such as metastases from a tumour. In these instances, a secondary investigation using MRI scans, CT scans or PET scans may be performed to look for other characteristics of the fracture as well as locate the source of a tumour if there was one.
If the fracture happened from trauma such as a road traffic accident or fall from height, the clinician would also examine other joints for associated injuries. An example would be a patient who fell from a height and has a fracture of his/her thigh bone; it would be prudent to exclude associated injuries of the hip, knee and even ankle.
Patients with open fractures will have visible open wounds that expose the bone to the environment. This puts the wound at a significant risk of getting infected. The management of patients with open fractures differs from that of closed fractures.
Treatment Options of Bone Fractures
- Non-surgical methods (casting, splinting)
If the fracture is undisplaced or even minimally displaced, the injured limb may be protected in a cast or sling to immobilise it so that it may heal naturally by itself. Most fractures take about 4 to 6 weeks to heal enough for patients to put weight on them. It may take another three months to mature fully. Patients are given medication to ease the pain and inflammation while they recover. Physiotherapy is also an important aspect of their recovery to help with function recovery and mobilisation.

Ankle fracture immobilised in a cast and crutches to help patients move around without putting their full weight on the injured ankle

Arm slings may be used to immobilise an injured shoulder for clavicle or some humerus fractures.
- Surgical interventions (internal fixation, external fixation)
Displaced fractures describe fractures which have shifted in position. This change may affect the function of the injured limb in the long run. The fracture may also worsen if patients move about during their daily activities. Surgical intervention is aimed at restoring the anatomy and function of the injured limb. This allows the patient to start their rehab earlier.

Surgical fixation of a proximal humerus (shoulder) fracture. Fixation includes the insertion of a titanium plate with screws. These implants are designed to stay in the patient forever. Depending on the location, the implants may be removed after a year or so. Removal of implants involves a second operation.
Some patients are involved in severe trauma and suffer from complex bone fractures and significant open wounds. These patients must be given intravenous antibiotics and tetanus injections as soon as possible to prevent infections. Due to the severity of the injuries, the affected limb is unstable and extremely painful.
An initial operation is performed to surgically clean the wounds and stabilise the fracture using external fixation.
External fixation describes the location of the metalwork outside of the skin. This technique involves small stab incisions to the skin, which helps preserve the soft tissue envelop and skin around the limb. The rods help to stabilise the injured limb. Once there is no further infection, orthopaedic surgeons may remove the external fixation after a while and stabilise the fracture using intra-medullary nails or plates which are buried under the skin.
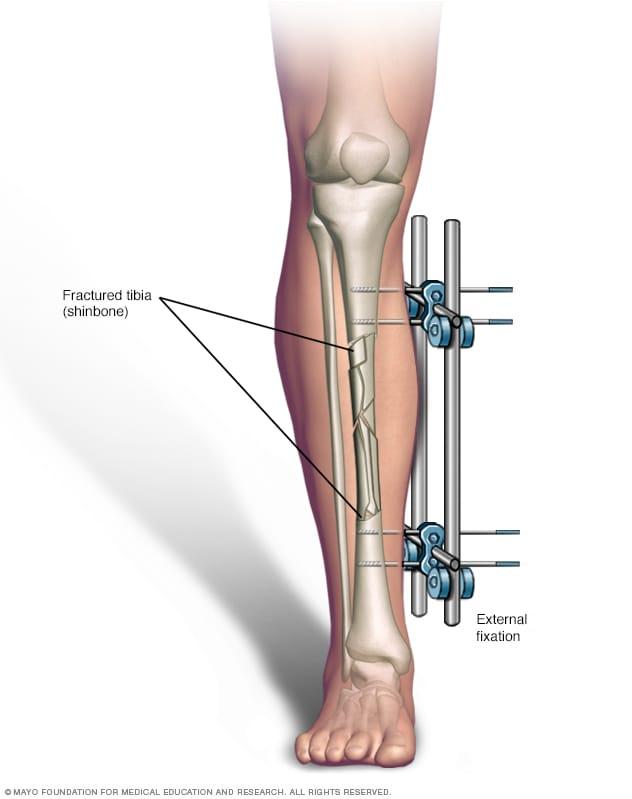
External fixation to stabilise the complex fracture of the tibia (shin bone). This operation is performed while patients are under general anaesthesia so they don’t feel any pain during surgery itself. It also allows a patient to move around with little discomfort since their fracture has been stabilised. External fixation is often just a temporary measure which is removed after a week or two.
Intra-medullary nails are used to stabilise fractures internally. The long nails are inserted into the medullary canals of the long bone and fixed with screws at the top and bottom of it. This prevents the nails from twisting or toggling around when patients move around. While these nails do not have to be removed, some patients prefer them out. This may be done after a year once the fracture has fully healed and matured. Removal of such implants is associated with specific risks and is not done routinely.

Strains and Sprains
Difference between Strains and Sprains
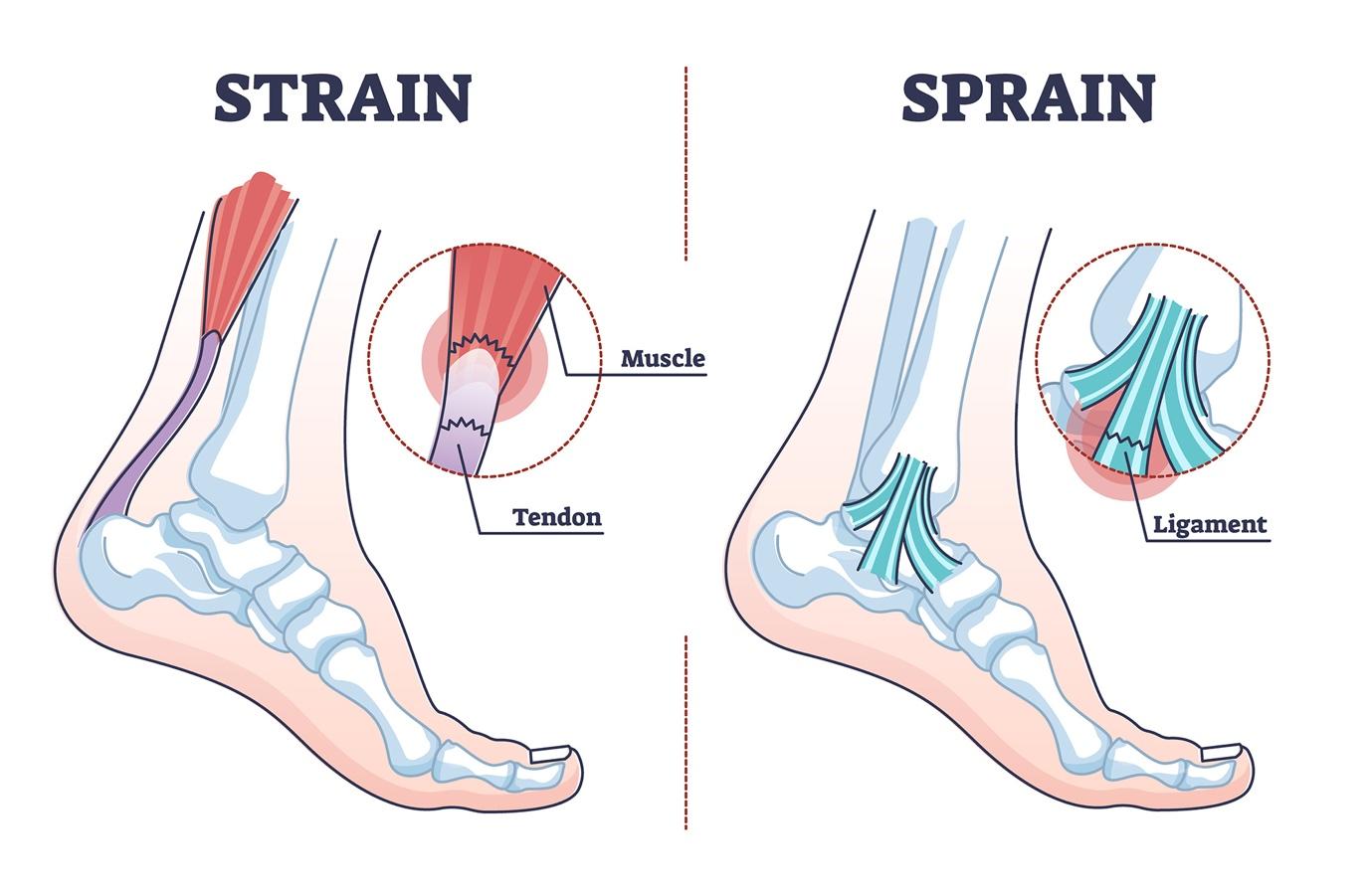
Sprains and strains may affect the same injured joint. However, it is important to understand the difference between the two injuries. It first begins with basic anatomy.
A tendon connects muscle to bone, while a ligament connects bone to bone.
Strains affect tendons and muscles, while sprains affect ligaments.
Commonly Affected Areas
Commonly affected areas include the ankle and shoulder.
Around the ankle, inversion injuries may cause partial or complete tears to the ligaments of the ankle e.g. ATFL.
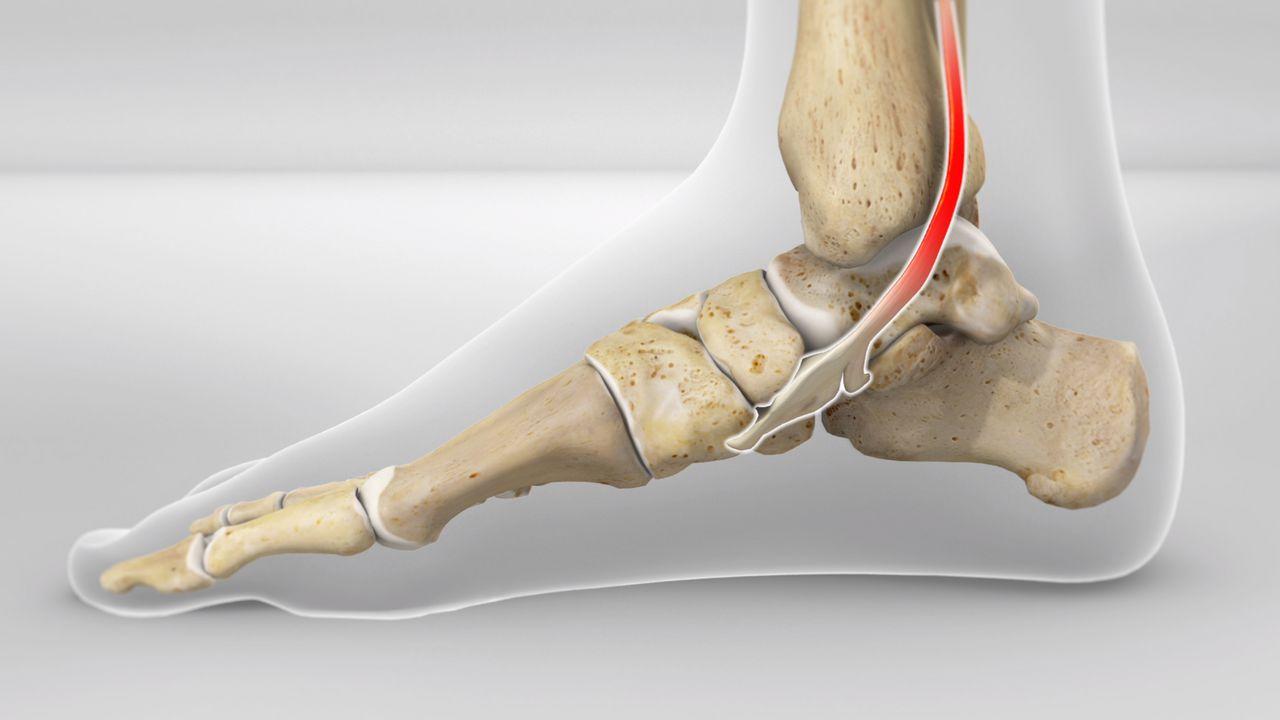
Strains due to jumping injuries may affect the Achilles tendon or peroneal tendons. Patients with flat feet may stress their ankles and cause inflammation to the tibialis posterior tendon.
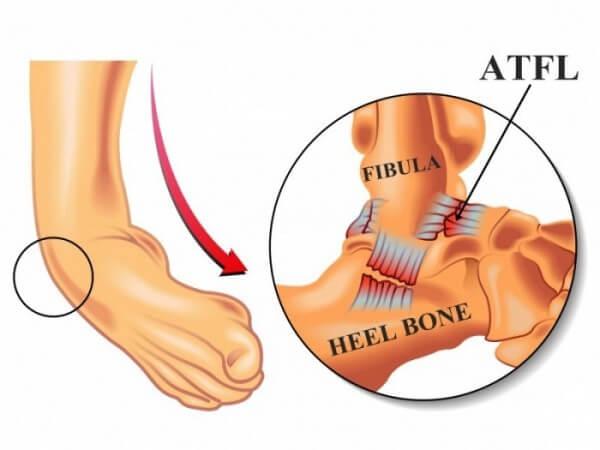
Inversion injuries of the ankle may cause rupture of the anterior talofibular ligament (ATFL) and other surrounding ligaments.
PTTD, or posterior tibial tendon dysfunction, is common in patients with flat feet. They experience pain around the back of the medial malleolus bone.
Around the shoulder, injuries to rotator cuff muscles and tendons are common. This is especially so for the supraspinatus tendon. This tendon glides between two bones: the acromium and greater tuberosity. Abrasion and constant impingement may cause the supraspinatus tendon to be inflamed, partially torn or completely detached and retracted.
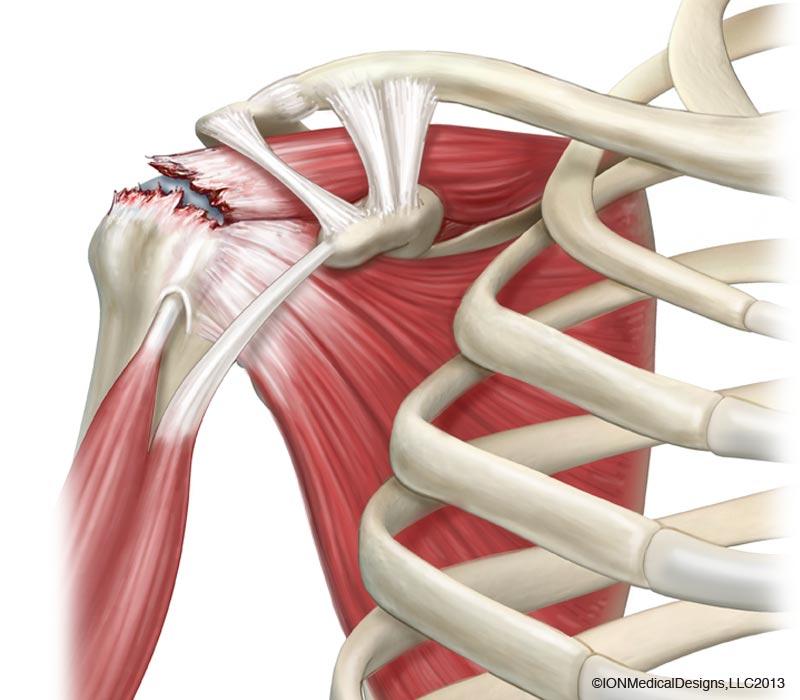
Supraspinatus tear in the shoulder may affect forward and sideward movement of the shoulder. If it is a complete tear, surgical reattachment may be required to restore function.
Strains & Sprains: Causes and Risk Factors
Shoulder and ankle sprains are very common sports injuries, especially in basketball, football and volleyball. Twisting and changing directions at speeds often cause ankle sprains. Those playing football on astroturf may find their studs stuck in the turf and tear the ACL in their knee.

Ankle sprains are common in basketball due to the sudden change in direction and landing awkwardly. May players land on someone else’s foot and sprain their ankle that way.
Volleyball players may experience shoulder injuries from repetitive movements and falls on an outstretched arm. Those who sustain these injuries outside of sports may sprain their ankle while walking on uneven ground or missing a step. Middle-aged patients may experience a tear in their rotator cuff tendon from doing house chores as their ligaments are not as stretchable and robust as before.

Shoulder injuries are common in volleyball due to repetitive movements, overstretching for the ball and landing awkwardly.
Symptoms and Diagnosis
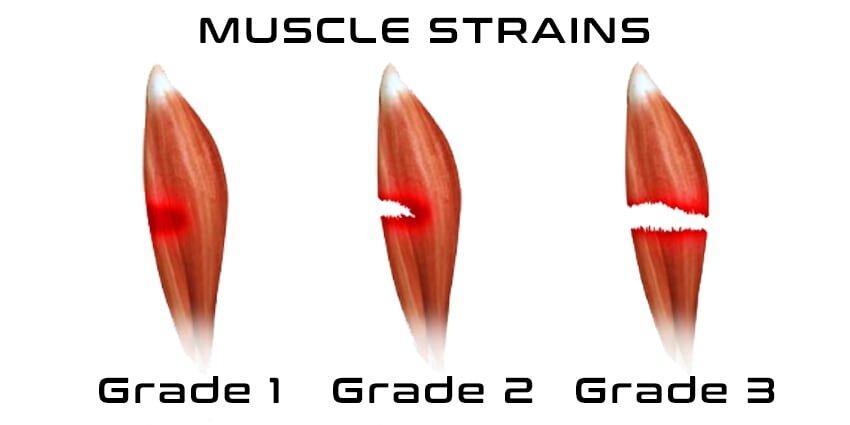
Minor strains may involve over-stretching of the muscles or tendons, while major injuries may include partial or complete tears of these tissues. During the initial stage of the injuries, patients may experience pain, bruising, swelling and loss of function. These symptoms often improve with rest, elevation, pain medication and compression. If the tendon is completely detached from the bone, surgical fixation may be required to restore function.
Most muscle and tendon injuries recover with conservative treatment.
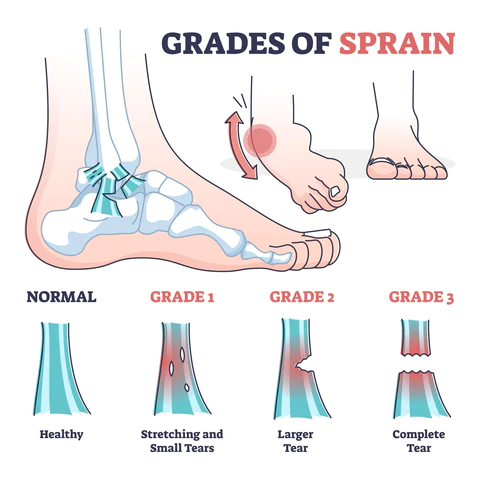
Sprains involve ligaments connecting bones to bones. Minor sprains recover after a week or two, while patients with more severe sprains may experience instability of their joints. They may not be able to walk on uneven ground if their ankle is unstable from a complete tear of their ATFL.
Treatment Approaches
- R.I.C.E. (Rest, Ice, Compression, Elevation)
- Physical Therapy and Rehabilitation
Initial resuscitation of the injured limb is important for good recovery. R.I.C.E. (Rest, Ice, Compression, Elevation) has always been the common teaching to manage such injuries. Compression, ice and elevation all help to control swelling. Less swelling equates to faster recovery. However, overly tight compression may limit blood flow and hinder natural healing. Early movement and weight-bearing are also important facets of recovery and rehabilitation. They help maintain muscle strength and joint flexibility.
Functional rehabilitation focuses on regaining the ability to perform daily functions and tasks. This should be facilitated by physiotherapists and rehab modalities such as ultrasound and cryotherapy treatments. Physical therapists help to reduce joint swelling and improve range of motion, muscle strength and balance of the limb. They also ensure patients have recovered well enough before their return to sport.
Tendonitis
Definition and Explanation of Tendonitis
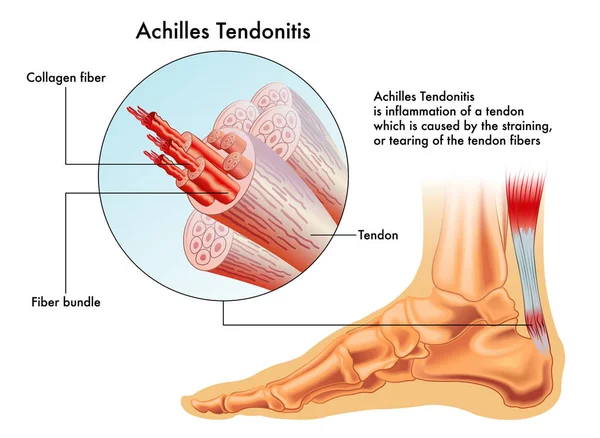
Tendonitis, a commonly encountered orthopaedic condition, is the inflammation or irritation of a tendon, the fibrous connective tissue that attaches muscle to bone. This condition results from repetitive overuse or sudden injury, leading to pain and reduced function in the affected area.
Most Affected Areas
Tendonitis is a condition that can strike various parts of the body, with some areas being more commonly affected than others. Among the most frequently encountered types is Achilles tendonitis, which causes discomfort and pain in the heel and lower calf, often affecting athletes and runners. Tennis elbow, formally known as lateral epicondylitis, leads to pain and tenderness on the outer side of the elbow, particularly in individuals who engage in repetitive gripping and wrist extension motions. Other prevalent areas of tendonitis include the shoulder's rotator cuff, which can result in impaired arm movement, as well as the patellar tendon in the knee, causing pain during activities like jumping or running. Wrist tendonitis, known as de Quervain's tenosynovitis, can impact the tendons on the thumb side of the wrist, leading to discomfort during hand and wrist movements. These conditions serve as a reminder of the importance of recognising and addressing tendonitis to ensure continued mobility and well-being.
Causes and Risk Factors of Tendonitis
Tendonitis often arises due to repetitive motions or overuse. Activities such as running, playing sports, typing, or lifting heavy objects can strain the tendons. Factors like poor posture, inadequate warm-up, and age-related changes in tendon structure also contribute to the risk of developing tendonitis. Individuals with certain medical conditions, like diabetes or rheumatoid arthritis, are at an increased risk.
Tendonitis: Symptoms and Diagnosis
The hallmark symptom of tendonitis is pain in the affected tendon. The primary indicators of tendonitis include:
- Pain in the affected tendon intensifies with movement.
- Impaired joint mobility.
- A sensation of grating or crackling when the tendon is in motion.
- Swelling is often accompanied by warmth or redness.
Diagnosis typically involves a physical examination, during which a healthcare provider assesses the affected area for signs of inflammation and discomfort. Imaging studies, such as X-rays or ultrasound, may be used to confirm the diagnosis and rule out other possible causes of pain.
Treatment Options for Tendonitis
- Rest and Activity Modification – Resting the affected area and modifying activities that aggravate symptoms are primary steps. This allows the tendon to heal.
- Physical Therapy and Stretching – Physical therapy can help with rehabilitation, strengthening the affected muscles, and improving flexibility. Specific exercises and stretches are tailored to each case.
- Anti-inflammatory Medications – Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can relieve pain and reduce inflammation.

An example of NSAID anti-inflammatory medication
In severe or chronic cases, where conservative treatments are ineffective, more invasive options like corticosteroid injections or surgery (in rare cases) may be considered. It is crucial to consult your doctor for proper diagnosis and guidance on the most suitable treatment plan. Moreover, prevention through adequate warm-up, proper technique, and ergonomic practices is essential in mitigating the risk of tendonitis and promoting long-term musculoskeletal health.
Preventive Measures
The Importance of Injury Prevention
Preventing orthopaedic injuries is paramount, as these injuries can significantly impact our quality of life, disrupt our daily activities, and hinder our mobility. Moreover, these injuries can lead to chronic issues if left unaddressed. By prioritising prevention through practices like proper body mechanics, regular exercise, as well as warm-up and cool-down techniques, we can reduce the risk of these injuries and maintain a higher level of physical well-being.
Tips for Reducing the Risk of Orthopedic Conditions
1. Proper Body Mechanics:
Proper body mechanics are fundamental for injury prevention. This minimises strain on the muscles and tendons, reducing the risk of orthopaedic issues. Below are some tips for posture and body mechanics:
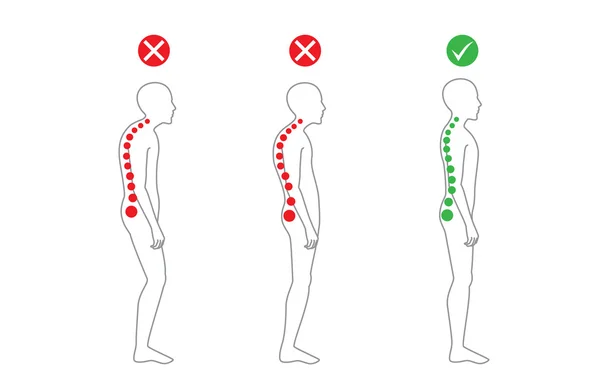
Correct alignment of body in standing posture
- Maintain proper posture by keeping the back and neck upright, shoulders relaxed, and minimizing twisting and bending.
- Position your work tasks directly in front of you.
- Maintain the right body position during activities, with close-to-body upper arms, 100-degree elbow angles, neutral forearms, and straight wrists.
- Avoid prolonged forward bending of the neck and use document holders for reading.
- Prevent muscle fatigue by avoiding static positions and promoting movement to enhance blood circulation.
2. Regular Exercise and Strengthening:
Developing strong muscles helps support your joints and reduce the risk of injuries. You may want to modify your workout routine to include exercises that target the muscles around your joints, such as leg lifts, squats, lunges, and core-strengthening exercises. It is best to seek advice from a fitness professional to tailor the exercises to your requirements.
3. Warm-up and Cool-down Techniques:
Warm-up and cool-down routines are essential before and after physical activity. A proper warm-up increases blood flow to the muscles, making them more pliable and thereby reducing the risk of strains and sprains. Stretching during a cool-down session helps maintain flexibility and reduces muscle tightness, enhancing overall joint health. Remember to get yourself warmed up before your stretch, as stretching cold muscles may result in injury. Stretch slowly and gently, and do not bounce or jerk your stretches. Breathe into your stretch to avoid muscle tension, and hold each stretch for 10 to 30 seconds.

Quadricep stretch
Below are some sample stretches:
- Quadricep (front of thigh) stretch
- Calf stretch
- Hamstring stretch
- Upper body stretch
- Tricep (back of upper arm) stretch
- Shoulder stretch
- Butterfly (inner thigh, hip and groin) stretch
- Lower back stretch
Incorporating these preventive measures into your daily routine is a proactive approach to minimising the risk of orthopaedic conditions. Remember that a healthy lifestyle, regular exercise, and attention to body mechanics can go a long way in preserving the integrity of your musculoskeletal system and ensuring a more active, pain-free future.